
Peer-led mobile crisis response refers to a wide range of services that are designed to meet the needs of community members experiencing crises related to mental health, behavioral health, or substance use. These services are deployed through the 911 emergency call system or a similar parallel system. Peer-led crisis mobile response aims to reduce police involvement in crisis calls, instead providing community members with direct access to professionals and paraprofessionals who can address their needs without the risk of escalation, arrest, or further violence.
Similar programs exist that do not include peers, but programs are much more successful when they prioritize leadership and care by peer providers who share life experiences with the community members they serve. Peer leadership and consensus-based decision-making are the necessary building blocks for on-going community accountability, since these elements preserve a care-based ethos both during service provision and among staff themselves.1Tim Black, CAHOOTS, Interview with Northampton Policing Review Commission, March 10, 2021; Rachel Bromberg, Reach Out Response Network, Interview with NPRC, January 5, 2021. https://www.youtube.com/watch?v=a1VP-DsHEs0 Shared experience among staff and clients helps build trust and also leads to care that is more responsive, compassionate, encouraging, and inspiring, enabling residents in distress to reach better outcomes and maintain more commitment to on-going self-care.2Davidson, Larry, Chyrell Bell Amy, Kimberly Guy, and Rebecca Miller. “Peer Support among Persons with Severe Mental Illnesses: A Review of Evidence and Experience.” World Psychiatry 11, no. 2 (June 2012): 123–28. https://doi.org/10.1016/j.wpsyc.2012.05.009
“Help isn’t help if it doesn’t help.”3Pat Deegan, quoted in Sera Davidow, for the Wildflower Alliance. “Open letter to the Mayor of Northampton,” May 19, 2021. https://wildfloweralliance.org/open-letter-to-the-mayor-of-northampton/
By contrast, negative contact with police (e.g. stops, arrests, incarceration) harms the well-being of the people involved. Research has documented a wide array of negative health outcomes from such interactions, including trauma, anxiety, psychological distress, worsening of chronic illnesses and substance-abuse conditions, and shortened life expectancy.4Sundaresh, Ram, Youngmin Yi, Brita Roy, Carley Riley, Christopher Wildeman, and Emily A. Wang. 2020. Exposure to the US Criminal Legal System and Well-Being: A 2018 Cross-Sectional Study. American Journal of Public Health 110: S116-S122. https://doi.org/10.2105/AJPH.2019.305414 These harms are not experienced equally by all community members. People of color, low-income residents, and other marginalized groups have disproportionately experienced heavy police presence and unwanted contact with police, high rates of arrest, and harsh enforcement tactics. People in distress due to mental or behavioral health crises are also often treated like criminals and threats to public safety, subject to enforcement and coercive, punitive medical interventions.5Irwin, Amos, and Betsy Pearl. The Community Responder Model. Center for American Progress, October 2020; Camplain, Ricky, Carolyn Camplain, Robert T. Trotter II, George Pro, Samantha Sabo, Emery Eaves, Marie Peoples, and Julie A. Baldwin. 2020. Racial/Ethnic Differences in Drug- and Alcohol-Related Arrest Outcomes in a Southwest County From 2009 to 2018. American Journal of Public Health 110: S85-S92. https://doi.org/10.2105/AJPH.2019.305409 Diverting non-violent emergency calls away from the police helps protect and build the well-being of community members while also alleviating the workload of the police department.
Yet as the communities most impacted by policing have made clear, reducing contact with police officers is not enough to guarantee compassionate care when you need it. Institutionalized social work and clinical models rely heavily on paternalistic and coercive interventions, collaborate with other harmful state institutions, and often have bad reputations with clients as a result. Peer-based care models instead draw on the wisdom and experience of survivors of state violence and psychiatric care. Peers “know what it is like to feel powerless over their own life,” in the words of the Wildflower Alliance.6Sera Davidow, for the Wildflower Alliance. “Open letter to the Mayor of Northampton,” May 19, 2021. https://wildfloweralliance.org/open-letter-to-the-mayor-of-northampton/ Peer models acknowledge the trauma caused by institutionalized care and offer consensual interventions that respect the humanity and autonomy of people in distress. These therapeutic practices are highly successful and even recognized internationally by the WHO, but they remain chronically under-resourced and under-utilized.7The World Health Organization promotes “rights-based transformation in mental health” and recognizes the Wildflower Alliance’s peer-based respite program as one of around 30 exemplary rights-based supports from around the globe. The WHO notes that policymakers and providers are calling for a “sea-change in mental health.”

Case study: CAHOOTS
The best-known example of peer-led crisis response is CAHOOTS (Crisis Assistance Helping Out On The Streets), a publicly-funded 911 response program run since 1989 by the White Bird Clinic in Eugene and Springfield, Oregon. When CAHOOTS is assigned a crisis call, they dispatch a two-person team consisting of a medic and a crisis worker. CAHOOTS response teams “deliver person-centered interventions and make referrals to behavioral health supports and services without the uniforms, sirens, and handcuffs that can exacerbate feelings of distress for people in crisis. They reduce unnecessary police contact and allow police to spend more time on crime-related matters.”8Beck, Jackson, Melissa Reuland, and Leah Pope. 2020. Case Study: CAHOOTS, Eugene, Oregon. Vera Institute of Justice. https://www.vera.org/behavioral-health-crisis-alternatives/cahoots Specifically, the teams provide services for:
- Crisis Counseling
- Substance Abuse
- Housing Crisis
- First Aid and Non-Emergency Medical Care
- Resource Connection and Referrals
- Suicide Prevention, Assessment, and Intervention
- Conflict Resolution and Mediation
- Grief and loss
- Transportation to Services
Responders focus on listening, empathizing, stabilizing, and de-escalating, especially prioritizing a person’s basic needs like warmth, food and water, shelter, compassion, and a sense of trust. Peer responders are trusted and have an established reputation for meeting people’s needs from a stance of “unconditional positive regard,” so that even the most tense situations become much more manageable. CAHOOTS response is also often an entry point for residents in distress to receive more sustained therapeutic services, helping them to reach a point of stability and well-being and reducing the need for future emergency response. Out of an estimated 24,000 calls CAHOOTS responded to in 2019, they called for police backup only 311 times (1.3% of calls). According to CAHOOTS, no staff member has ever experienced a serious injury in over 30 years of responding to emergency calls.
75% of CAHOOTS responders identify as peers with lived experience of incarceration, substance use, neurodivergence, houselessness, and other forms of oppression. This level of peer participation is key to CAHOOTS’s success: because their staff positions are non-licensed paraprofessionals who get extensive on-the-job training, it’s easier for people from diverse backgrounds to get hired. Non-licensed crisis workers are also unable to involuntarily hospitalize community members, which greatly increases trust by residents in crisis.
The White Bird Clinic itself is run as a consensus-based collective with a diverse “stewardship council” made up of residents from the communities they serve. CAHOOTS thrives because of community trust, and that trust is built on providing care that is compassionate and consensual, unlike the punitive and coercive approaches that police and social workers rely on.
Impact on 911 response and city finances
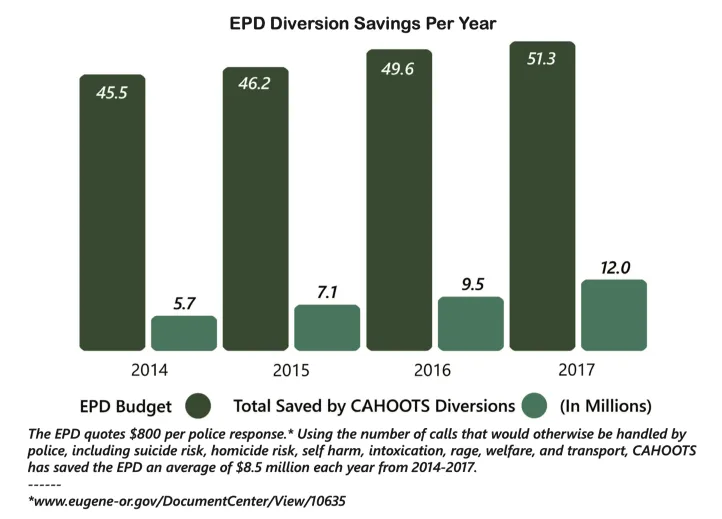
In Eugene and Springfield, CAHOOTS handles 20% of 911 calls, despite having a budget that is only 2% of the police budget. CAHOOTS costs approximately $70/hour for emergency response, whereas police emergency response ranges from $200-300/hour. With a budget of only $2.2 million, CAHOOTS is estimated to directly save the municipalities $14 million. The program also saves hospital and health system costs by diverting emergency room visits and providing transportation as necessary. The Center for American Progress estimates that the CAHOOTS model could offer significant additional benefits and savings if they expanded their services to other low-risk non-emergency calls, diverting as much as 38% of 911 calls depending on local conditions.9Irwin, Amos, and Betsy Pearl. The Community Responder Model. Center for American Progress, October 2020.

Peer-led crisis response offers benefits to police, as well, reducing the burden that non-violent emergencies put on departments and improving community trust. Increasingly since the advent of the 911 emergency call system, police have become the default mode of response to any call for help, expanding the scope and cost of policing and causing significant collateral damage in communities–especially among marginalized groups. As former Dallas Police Chief David Brown said:
“We’re asking cops to do too much in this country… Every societal failure, we put it off on the cops to solve. Not enough mental health funding…loose dogs…schools fail… Policing was never meant to solve all those problems.”10Dennis, Brady, Mark Berman, and Elahe Izadi. “Dallas Police Chief Says ‘We’re Asking Cops to Do Too Much in This Country.’” Washington Post, July 11, 2016.
Making it happen in Greenfield
This proposal and the example of CAHOOTS are not an exact blueprint for a crisis response program in Greenfield. CAHOOTS helps us to see what’s possible when peer models are supported and allowed to take on big responsibilities, but any program we build will have to be developed by the community and local partners, taking into account our local needs, capacities, and resources. We are blessed with local organizations who are recognized leaders in peer support and harm reduction. Greenfield city government must support them and help build their capacity, rather than crowding them out with inappropriate, harmful interventions.
It’s time to convene these conversations. Together let’s take concrete steps towards shifting the paradigm of crisis response in our community.
Greenfield People’s Budget
June 2021
Further resources
The following resources offer more detail on CAHOOTS and similar programs, implementation considerations, and comparisons with other response models.
- More about CAHOOTS – videos & articles
- The Wildflower Alliance’s Open Letter to the Mayor of Northampton, May 19, 2021
- Implementing Peer-Led Crisis Response – reports for municipal officials
- 1Tim Black, CAHOOTS, Interview with Northampton Policing Review Commission, March 10, 2021; Rachel Bromberg, Reach Out Response Network, Interview with NPRC, January 5, 2021. https://www.youtube.com/watch?v=a1VP-DsHEs0
- 2Davidson, Larry, Chyrell Bell Amy, Kimberly Guy, and Rebecca Miller. “Peer Support among Persons with Severe Mental Illnesses: A Review of Evidence and Experience.” World Psychiatry 11, no. 2 (June 2012): 123–28. https://doi.org/10.1016/j.wpsyc.2012.05.009
- 3Pat Deegan, quoted in Sera Davidow, for the Wildflower Alliance. “Open letter to the Mayor of Northampton,” May 19, 2021. https://wildfloweralliance.org/open-letter-to-the-mayor-of-northampton/
- 4Sundaresh, Ram, Youngmin Yi, Brita Roy, Carley Riley, Christopher Wildeman, and Emily A. Wang. 2020. Exposure to the US Criminal Legal System and Well-Being: A 2018 Cross-Sectional Study. American Journal of Public Health 110: S116-S122. https://doi.org/10.2105/AJPH.2019.305414
- 5Irwin, Amos, and Betsy Pearl. The Community Responder Model. Center for American Progress, October 2020; Camplain, Ricky, Carolyn Camplain, Robert T. Trotter II, George Pro, Samantha Sabo, Emery Eaves, Marie Peoples, and Julie A. Baldwin. 2020. Racial/Ethnic Differences in Drug- and Alcohol-Related Arrest Outcomes in a Southwest County From 2009 to 2018. American Journal of Public Health 110: S85-S92. https://doi.org/10.2105/AJPH.2019.305409
- 6Sera Davidow, for the Wildflower Alliance. “Open letter to the Mayor of Northampton,” May 19, 2021. https://wildfloweralliance.org/open-letter-to-the-mayor-of-northampton/
- 7The World Health Organization promotes “rights-based transformation in mental health” and recognizes the Wildflower Alliance’s peer-based respite program as one of around 30 exemplary rights-based supports from around the globe. The WHO notes that policymakers and providers are calling for a “sea-change in mental health.”
- 8Beck, Jackson, Melissa Reuland, and Leah Pope. 2020. Case Study: CAHOOTS, Eugene, Oregon. Vera Institute of Justice. https://www.vera.org/behavioral-health-crisis-alternatives/cahoots
- 9Irwin, Amos, and Betsy Pearl. The Community Responder Model. Center for American Progress, October 2020.
- 10Dennis, Brady, Mark Berman, and Elahe Izadi. “Dallas Police Chief Says ‘We’re Asking Cops to Do Too Much in This Country.’” Washington Post, July 11, 2016.